Neisseria
CASE 1
• A 19 year old man has burning pain with urination for 36 hours. He has noted a discharge from his penis that produces yellow spots on his underpants. The patient has no fever, chills, or sweats and no other pain.
• The patient comes from a village in the Volta region where his primary family lives and where he attended high school. He has moved to Accra to work in a local hotel. He is currently living with two cousins from his village. During the past month, he has had two female sexual partners, one of whom he considers to be a steady girlfriend.
• On physical examination, he is afebrile and his vital signs are normal. On the genital examination, the patient has a yellow-white penile discharge (see below left). There are no genital ulcerations. There is no testicular or epididymal enlargement or tenderness to palpation, and there are no enlarged inguinal lymph nodes.
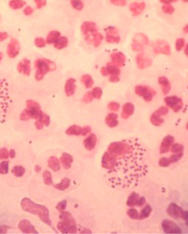
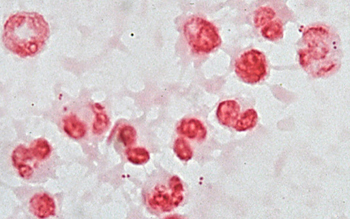
• A Gram stain of the penile discharge shows Gram-negative intracellular diplococci (below right).

• The patient is treated with ciprofloxacin and doxycycline.
Questions:
1. The intracellular Gram-negative diplococci belong to which species?
2. How was this infection acquired?
3. Once acquired, what was the probability that the patient would have symptoms?
4. If this condition is not treated, what are the potential consequences?
5. None of the patient's sexual contacts have symptoms. Why? Should they be treated anyway?
6. Should the patient be tested for HIV also?
7. After this infection, will the patient be immune? What mechanisms of of this organism prevent the development of protective immunity?
8. What tissues and which cells will this organism infect in the male and female hosts?
9. Why has it been difficult to develop an effective vaccine for this pathogen? What mechanisms of this pathogen prevent the development of protective immunity?
CASE 2
• A 20 year old woman has increasing lower abdominal pain for 3 days. The pain began insidiously, but now she is unable to walk comfortably. She has had a few chills, but no rigor (shaking). She is nauseated and vomited once this morning. She developed a mild vaginal discharge during the past week. A review of her polyclinic chart indicates that she was also treated 4 months ago for mucopurulent cervicitis. The past history is otherwise unremarkable.
• The patient has had two recent sexual contacts. She is unaware that either has had any STD.
• Her temperature = 37.8C, heart rate = 96/min. The abdomen is not distended, and there are normal bowel sounds. There is diffuse lower quadrant tenderness with mild rebound noted in the right lower quadrant.
• A pelvic examination is performed. There is mucopus seen at the cervical os. On palpation, there is exquisite pain with any manipulation of the cervix, and there is fullness and tenderness in the left adnexa, presumably an enlarged Fallopian tube.
Questions:
1. This infection likely involved N. gonorrhoeae at some point, and it may be present now. What other microorganisms might be involved in this current infection?
2. What culture media would be required to isolate N. gonorrhoeae from this patient's mucopus? What does the media contain? What is chocolate media? What is Thayer-Martin media? What is the difference between the two?
3. What simple laboratory test distinguishes this pathogenic Neisseria from non-pathogenic Neisseria in culture?
4. What long-term complications may occur as a result of this infection?
5. Should this patient's male sexual partners be treated? or examined?
6. Should the patient be tested for HIV? If so, why?
CASE 3
• A 14 year old male has fever, severe headache, and stiff neck since awakening this morning. He is brought to the Emergency Department from his boarding school 12 hours after the onset of symptoms.Two other students from the school have similar illnesses that began on the same day.
• His temperature is 38.9 degrees. His mental status is normal, and a cursory neurological examination reveals no focal abnormalities. However, there is profoound stiffness of his neck. With passive anteflexion of the neck, he actively bends and raises his knees.
• A lumbar puncture is performed promptly, and it yields slightly turbid fluid. A Gram stain of the fluid shows neutrophils with occasional Gram-negative diplococci (some intracellular).
Questions:
1. What is this organism? How was it acquired?
2. How would you culture the spinal fluid to recover this organism?
3. What is the principle virulence factor of N. meningitidis that is not shared by N. gonorrhoeae?
4. What will happen to the patient if he does not receive antibiotic treatment? Why?
5. For treatment to be successful, the antibiotic used must have which essential characteristics?
6. Are the patient's healthy roommates at any risk of developing this disease? If so, what should be done for them?
7. What type of vaccine is protective against this disease? Are there any variants of N. meningitidis for which vaccine is not effective?